Information for Parents, Educators and Allied Health Professionals
The successful collaboration of educators, allied health professionals and the Autistic community (Autistic individuals and their loved ones), has led to a wealth of early interventions that have demonstrated significant therapeutic outcomes for Autistic Children.
Promoting acceptance
Guidepost One: Celebrate Inclusive Practices
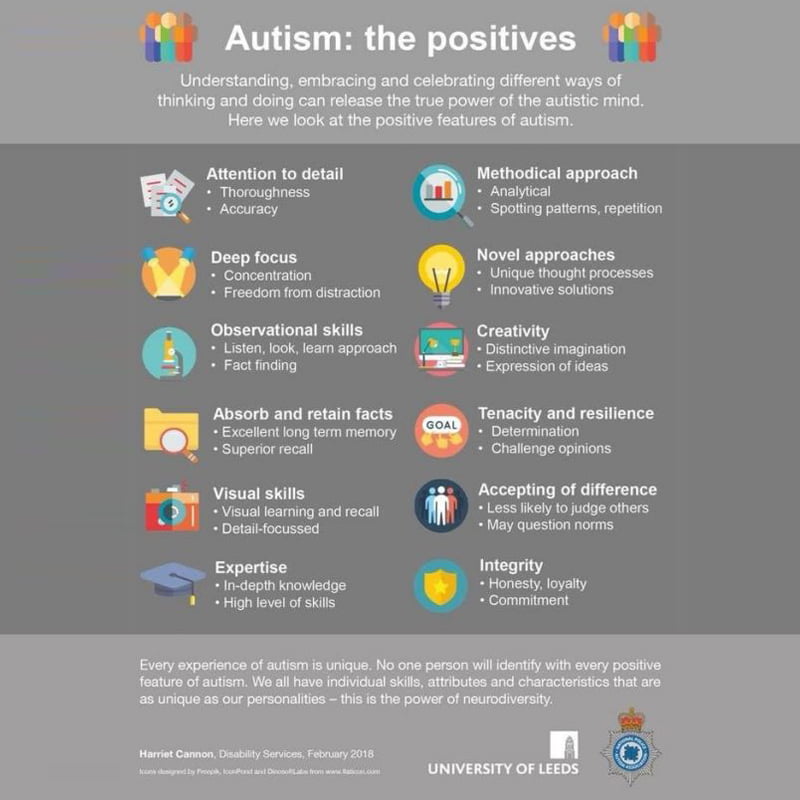
Autistic children often have a zest for learning and are fascinated by facts. Their acute sensitivity to sensory experiences and stimuli gives them a remarkable view of the world. Connections (as distinct from socializing, which is internalizing social norms) provide meaning in relationships—whether with people, objects, or stimuli.
Autistic children can often focus intently and learn a lot about topics they are especially interested in. Encouraging special interests is a highly effective way to engage students who present with an interest-based nervous system. If the child is disengaging or becoming distressed, consider if the child is having difficulty processing oral language. A lot of information in the classroom in presented orally, and it is important to provide visual schedules and visual learning strategies. An example of helping a student with executive functioning may include a visual support for task analysis.
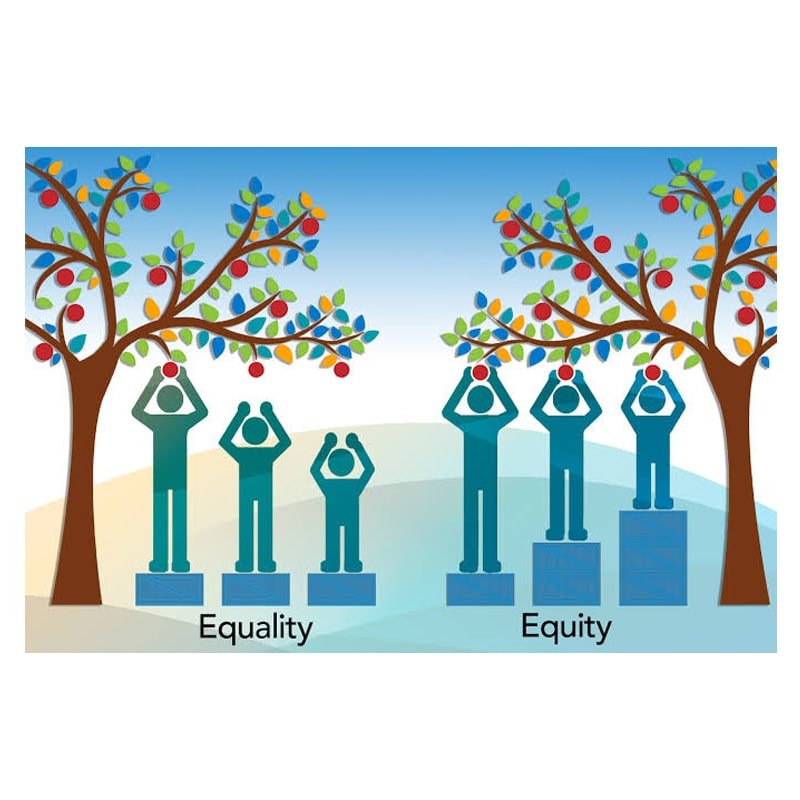
In addition to autistic individuals developing new skills to promote their well-being, acceptance and understanding from others is essential. A diagnosis of autism spectrum disorder can allow neurodiverse individuals to stand with pride and connect to their tribe. By offering, respect, support, and flexibility (accommodations in the workplace and education system), we will encourage self-determination, empowerment, and innovations for the good of all.

Guidepost Two: Navigate with Emotional Attunement
Dr. Stephen Porges has coined the term neuroception, which describes how our neural circuits distinguish whether stimuli are safe or dangerous. Specific areas of the brain detect and evaluate features such as body and facial expressions and environmental triggers to evaluate an impression of safety or trustworthiness. In looking through the lens of polyvagal theory we can understand that although an environment may not appear to be threatening (e.g., a noisy, busy, brightly lit classroom), the neuroceptive circuits of a neurodivergent individual may be triggered. A neuroception of safety is necessary before social engagement behaviours can occur.
Autistic individuals are susceptible to emotional contagion (the tendency to absorb, catch, or be influenced by other people’s feelings). An autistic child can distinguish very subtle cues that others would not. Professor Tony Attwood described this as a sixth sense and likened this experience to the analogy of a negative tone of voice infecting a neuro-typical person at the strength of a cold. In contrast, the autistic child is infected at the strength of the flu. This can be an overwhelming experience for an autistic child.
Emotional dismissal and/or misattunement is crippling for autistic children who cannot easily bypass contempt and strongly need a deep and authentic connection. Autistic children are highly aware of their surroundings and need someone to validate their experiences. Demonstrating emotional attunement (a desire to understand and an ability to respect the child’s inner world) influences social and emotional development (self-regulation, attachment, and a sense of self).
A sense of safety (i.e., a visceral feeling of safety) requires both a reduction of cues of danger and the experience of cues of safety (Porges, 2009). Polyvagal theory provides us with a sophisticated understanding of why focused attunement with another person can shift us out of disorganized and fearful states (Porges, 2009).
When the autonomic nervous system has moved into a dysregulated dorsal vagal state (shutdown, numbing, disconnection, or dissociation) or sympathetic state (mobilization of fight or flight, survival mode thinking), a quest for safety and connection can be realized by co-regulation (Dana, 2020). Co-regulation is defined as the way in which one person’s autonomic nervous system interacts with another person’s autonomic nervous system in a way that facilitates connection and safety.
This involves a recognition of a shift in one’s autonomic state, which is met with a responsive, warm, calming presence and tone of voice. In order to facilitate co-regulation, you need to honor the person’s experience (i.e. you are not trying to resolve or escape from the emotion, rather you are emotionally attuned to meeting them where they are at). Co-regulation is dependent upon how the person is seen, heard, held and the ways they are offered safety and connection (Dana, 2020).
When an Autistic child is tired and overwhelmed it may feel like they pre-set and practice for what could happen at any given moment.

Please don’t assume a parent is being lax by not picking up on every little thing. Things need to be worked on in ways that are conducive to the child (intervention is likely needed) and only when the child is in the right head space to do so. Remember families are doing their best on any given day and the struggle can be invisible. A child’s parent is a valuable resource, as they know their child best. A good teacher will tell you where to look, however they will not insist on what you must see. This is greatly appreciated by parents of children with special needs.The reality of most Autistic individuals/families is a calendar full of appointments that may range from Occupational Therapy, Speech Therapy, Psychology, Dietician, Physiotherapy, Paediatrician, early intervention, support plans, multi-disciplinary meetings, group therapy, private swimming lessons etc.

Hope, perseverance, and flexibility are crucial in supporting people who feel the weight of symptoms of Autism Spectrum Disorder as they work incredibly hard to centre the mind and body.
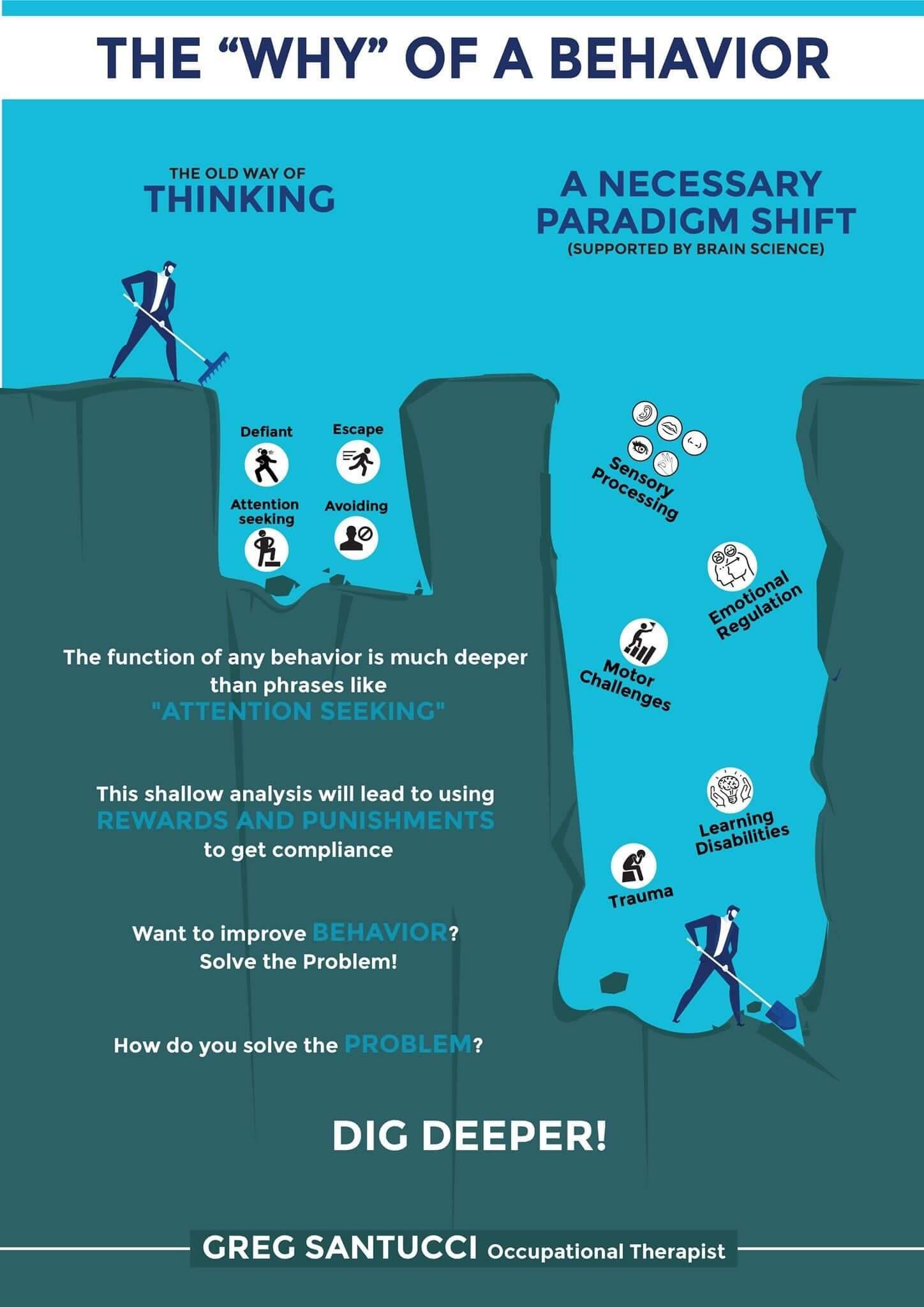
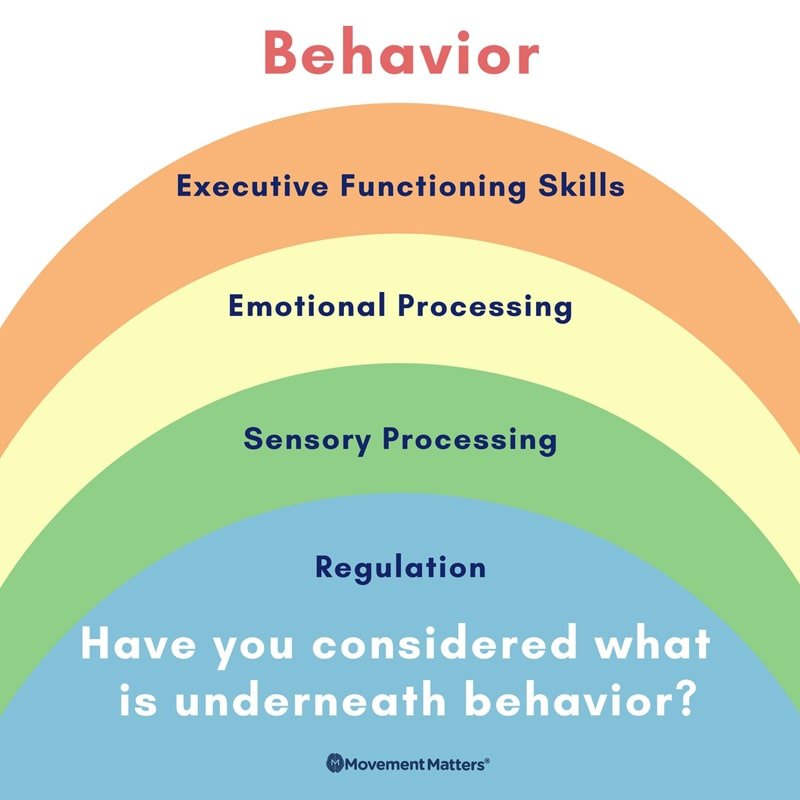
Dr Mona Delahooke discusses in her book ‘beyond behaviours’, the implementation of Neuro-biologically informed treatment models. Dr Delahooke provides an opportunity for an understanding of the brain/body connection, which has profound implications for how we understand, treat and support behavioural differences in Autistic children. Dr Delahooke supports development with a view that is respectful and inclusive.
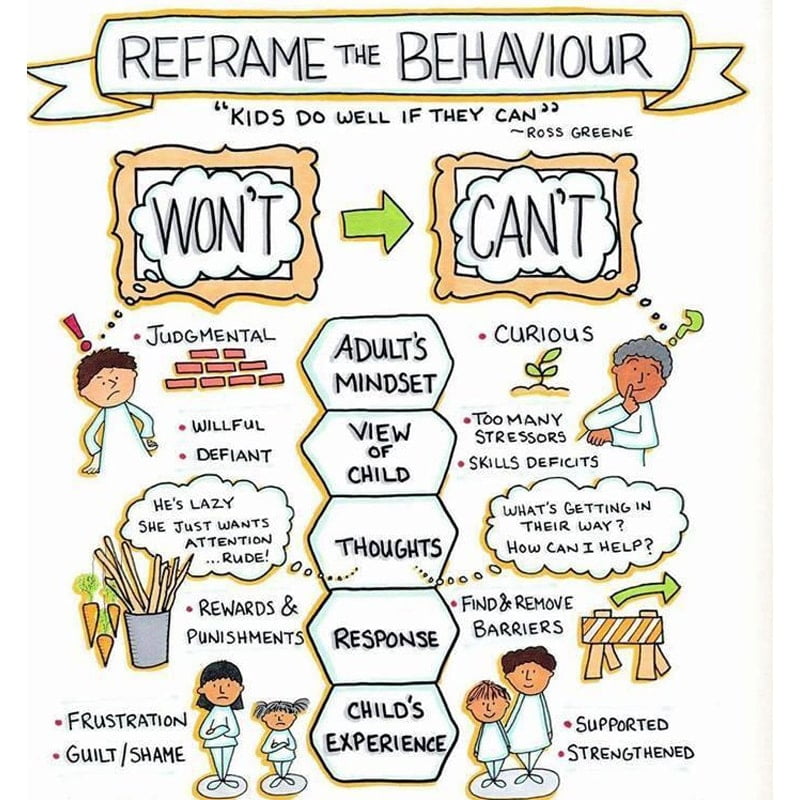
Please find below a link to learn the basics of the collaborative and proactive solutions (CPS) model, by Dr Ross Greene. https://livesinthebalance.org/walking-tour/
The CPS model is the evidence-based model of care that helps to focus on identifying the problems that are causing concerning behaviours in kids and solving those problems collaboratively and proactively.
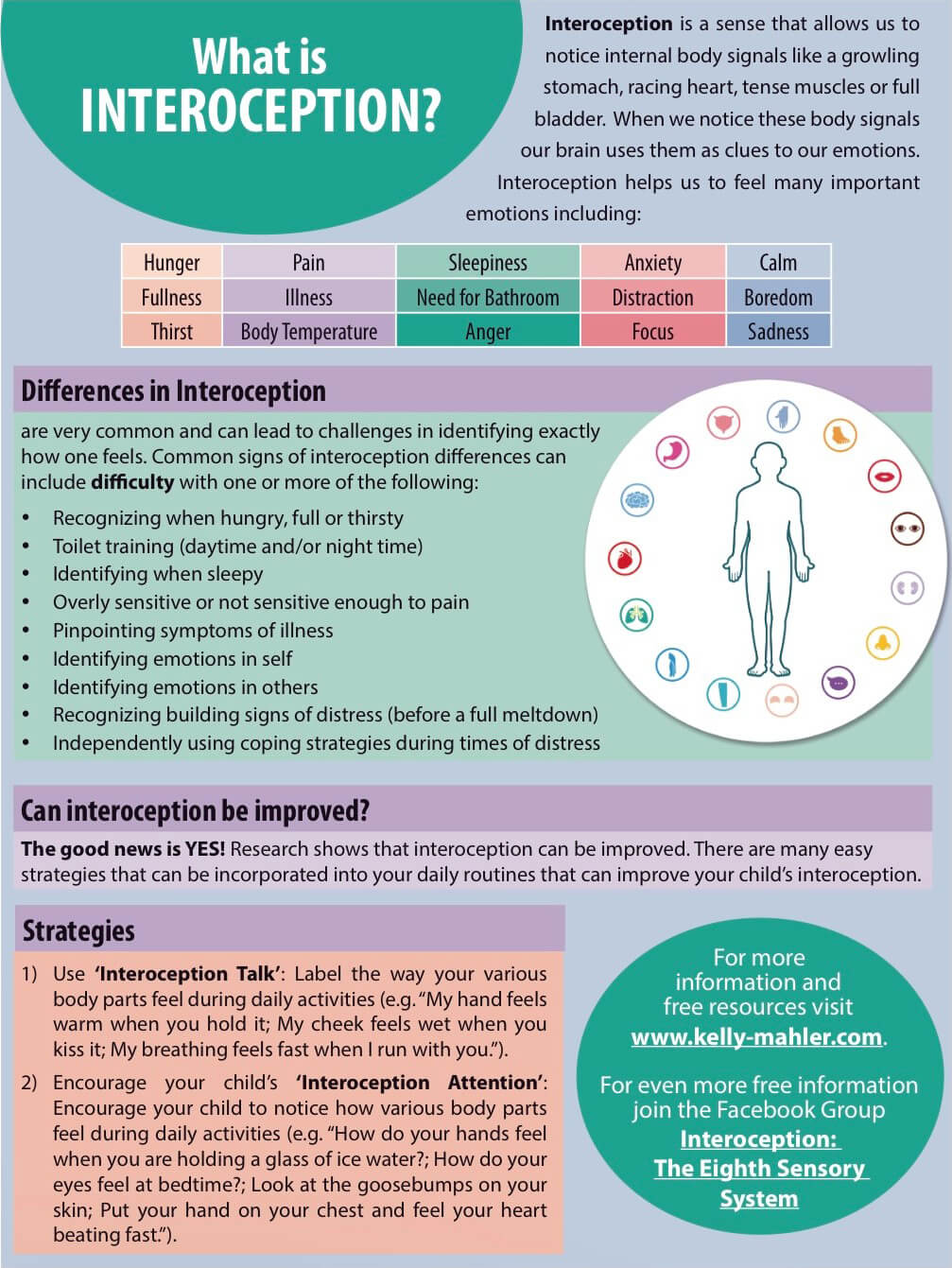
Please see below evidence-based supports that facilitate discovery and validation of each person’s unique interoception experience which in turn empowers people with self-understanding, self-regulation, health, well-being and social connection.
https://www.kelly-mahler.com/
It has been thoroughly discredited that Autistic individuals lack empathy. Research indicates that Autistic individuals possess difficulties with self-understanding and theory of mind, however not with affective empathy (Dziobeket., 2007). Autistic individuals are very sensitive to the emotional energy (sensitivity to other people’s moods) in a room and/or tone of voice. The Autistic Child can distinguish very subtle cues that others would not (sensitive empathic attunement). Professor Tony Attwood describes this as a sixth sense and likened the experience to the analogy of a negative emotion infecting a neuro-typical person at the strength of a cold, whereas the Autistic child is infected at the strength of the flu. This can be an overwhelming experience for an Autistic child. While all children must learn to emotionally self-regulate, this skill is critically important for Autistic children, as they are more susceptible to emotional contagion (the tendency to absorb, catch or be influenced by other people’s feelings). Emotional dismissal and/or misattunement are crippling for Autistic children who cannot easily bypass contempt and strongly need a deep and authentic connection. Autistic children are highly aware of their surroundings and need someone to validate their experience.
Dr. Stephen Porges has coined the term neuroception, which describes how our neural circuits distinguish whether stimuli are safe or dangerous. Specific areas of the brain detect and evaluate features such as body and facial expressions and environmental triggers to evaluate an impression of safety or trustworthiness. In looking through the lens of polyvagal theory we can understand that although an environment may not appear to be threatening (e.g., a noisy, busy, brightly lit classroom), the neuroceptive circuits of a neurodivergent individual may be triggered. A neuroception of safety is necessary before social engagement behaviors can occur. A sense of safety (i.e., a visceral feeling of safety) requires both a reduction of cues of danger and the experience of cues of safety (Porges, 2009). Polyvagal theory provides us with a sophisticated understanding of why focused attunement with another person can shift us out of disorganized and fearful states (Porges, 2009). Demonstrating emotional attunement (a desire to understand and an ability to respect the child’s inner world) influences social and emotional development (self-regulation, attachment, and a sense of self).
Autistic children experience subclinical inabilities to identify, label and describe emotions. Research indicates that a large proportion of Autistic individuals present with Alexythymia (Hill and Berthoz, 2010). Professor Tony Attwood suggests eloquent expression of music, lyrics, poetry, typing, email, or art to understand the individual persons experience.

Understanding the Significance of a Hyper Sensitivity to Sensory Experiences and Autistic Burnout
Understanding the Significance of a Hyper Sensitivity to Sensory Experiences and Autistic Burnout
Please do not remove sensory breaks due to the child no longer asking for them. Autistic adults continue to need sensory breaks and report how helpful and necessary it is to rest, recover and recharge.

Guidepost Three: Masking Goals Are Adverse for Mental Health
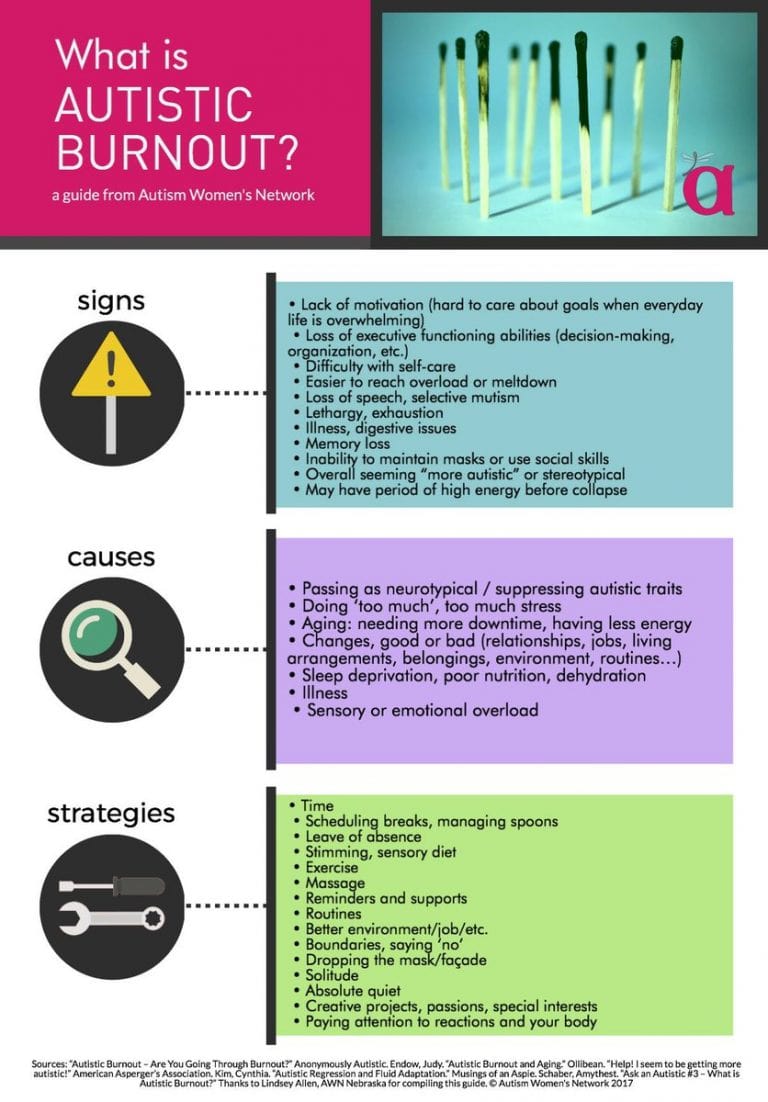
Many Autistic children learn to mask their behaviours to fit in and be accepted by their peers and/or due to an assumption that neurotypical social skills are the only way to succeed in life. Time off without the mask is not only physically and emotionally exhausting (which can lead to burnout), it is particularly adverse for mental health (anxiety, depression), self-perception and self-esteem. Time spent without ‘masking’ and a passage of time to recover, may be needed.
An important first step to removing the mask is one of acceptance, before we can identify and embrace the many strengths and beauty of the Autistic person. When we can come to accept our whole selves, we can remove the mask that makes us feel hidden, rejected and disconnected.
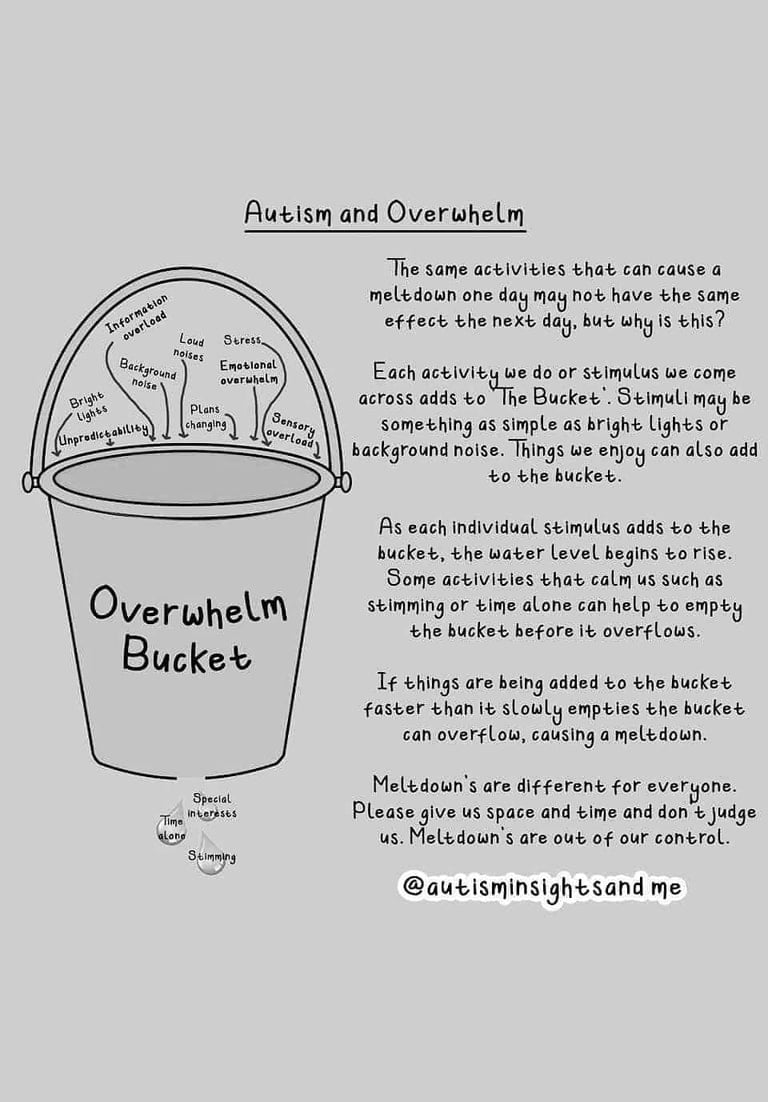
If a child is experiencing symptoms of autistic burnout, they may appear to regress—becoming less flexible in their thinking and reaching meltdown more easily—and will present with increased reactivity (e.g., behavioral concerns). An analogy I often use to explain this to adults is that the child’s cup is full; the addition of any further stimuli leads to a dysregulated state.
When the social demands outweigh the child’s ability to cope, meltdowns present as the autonomic state of a dysregulated dorsal vagal state (shutdown, numbing, disconnection, or dissociation), or a sympathetic state (mobilization of fight or flight, or survival mode thinking). This may have resulted from the combination of a lack of accommodations, sensory and/or emotional overload, insufficient opportunity to feel diverse thinking skills are of value, and/or suppressing autistic traits.
While self-care is a particularly important approach for treating symptoms of burnout (a balanced diet, sleeping, creating opportunities for being vs. doing, etc.), what is essential for treating autistic burnout is increasing the level of accommodations to ensure the environment is more in sync with the child’s needs. Activities that are regulatory, rhythmic, and/or involve movement are beneficial for completing stress cycles (to help the body move out of survival mode thinking). Neurodivergent minds need to rest and recharge. There are many different types of rest, including sensory rest, creative rest, emotional rest, and social rest.
You can teach a person to repress their emotions and not react (they are no longer disrupting anyone) however what you don’t see is how much you are hurting the Autistic person. They may go home and scream for hours, have nightmares, physical symptoms (eg. Migraines or IBS) exhaustion (be incapable of leaving the house and needing to do nothing except sleep), experience escape ideation (suicidal thoughts, self harm), burnout etc. Please be compassionate. Please do not deny a child the right to leave a situation if it leads to physically discomfort and/or if they are exhausted. Just being in a classroom with bright lights, noises, transitions etc. can be exhausting.
Co-regulation is dependent upon how the child is seen, heard, and offered a neuroception of safety—i.e., a reduction of cues of danger and the experience of cues of safety via connection (Porges, 2009). Demonstrating emotional attunement (a desire to understand and an ability to respect the child’s inner world) influences social and emotional development (self-regulation, attachment, and a sense of self). In her book Beyond Behaviors, Dr. Mona Delahooke discusses the implementation of neuro-biologically informed (i.e., understanding the brain/body connection has implications for supporting behavioral differences in autistic children) treatment models that are respective and inclusive.
In order to support future generations of neurodiverse children from experiencing the adverse impact of autistic burnout, it is important that we move towards a neuro-affirming and neuro-biologically informed approach that accommodates to the level of the child’s individual needs.
Please find below links that describe Autistic Burnout and the adverse impact of Masking
Exposures alone will not always work (You must address the symptoms of Autism):
As with any child, if they become controlling of their environment as a way of coping (which is not due to symptoms of Autism Spectrum Disorder) then it may be beneficial to continue with an exposure to allow the child to develop skills or strategies so they can manage their emotions when faced with such triggers. For example, all children need to learn to sit with their emotions until they dissipate on their own accord and cope with triggers that are unavoidable for later success socially, emotionally and academically.
Unlike a neurotypical child, repeated exposures to a situation will not always benefit an Autistic child. In fact, repeated negative exposures will do more harm than good. The symptoms of Autism Spectrum Disorder must be addressed, and developmental gains also need to be considered. The distinction I make about being more flexible is if it is a hypersensitivity that is making the child feel overwhelmed or if they can’t understand or cope with a situation because their brain works differently. In these situations, you must address the symptoms of Autism Spectrum Disorder, by providing a therapeutic intervention and/or appropriate accommodations (e.g. a social story to help understand what is expected of them).
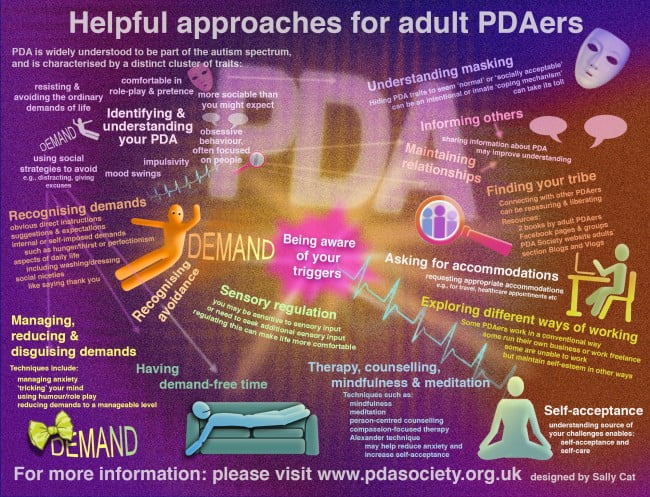
Pathological demand avoidance is characterised by an overwhelming need to avoid or resist demands, due to past negative experiences or burnout.
Innovative Ideas Designed by Autistic Children
Judgemental Assumptions are Not Helpful
Insights about Autism
Written by Erin Bulluss, Ph.D., and Abby Sesterka – Published in Psychology Today
Please find below Articles Written by Parents of Autistic Children

Distinguishing Empathy vs. Theory of Mind
Empathy is a recognition and understanding of the states of mind of others, including their beliefs, desires, and particularly emotions. While empathy is known as emotional perspective-taking, theory of mind is defined as cognitive perspective-taking (the ability to understand that others have beliefs, desires and intentions that are different to one’s own). A young Autistic child may become upset if someone does not know the answer to a question or experience difficulty with anticipating what others will say or do in a variety of situations.
From years of clinical practice, I have learnt that Autistic individuals experience deep empathy, so much so that they often cannot watch the news as they are distressed by what happens in the world and as small children this level of empathy is beyond compare (so much so that they become highly distressed by the suffering of others).

Accommodations in Schools may Include (This is by no means an exhaustive list)
*Please note the following supports are dependent on diagnosis, resources and funding
A diagnosis of Autism Spectrum Disorder provides understanding, resources and support. Early intervention is crucial to ensure that your child is receiving adequate treatment and support for perceived skill deficits. Therapy Based Interventions focus on communication, social development and sensory motor development.
If you child has a disability or learning need, they are entitled to a student support group meeting every term and individual learning plan. The goals of an Individual Plan are to document the child’s strengths and needs identified through a collaborative process with a multidisciplinary team of educators, allied health or early intervention providers, and the family. The plan will incorporate how the specified goals will be achieved (e.g. reasonable adjustments for the student), monitored and reviewed accordingly. Please find below a link for more information.
YLB De Mental Health Resource Digital
Reasonable adjustments | Association for Children with Disability (acd.org.au)
I CAN Network – I CAN Network Ltd
Autism & Aspergers Tutoring – How we support students with ASD | Cluey (clueylearning.com.au)
Spotlight On Supporting Autistic Girls at School
Square Peg Round Whole Podcast
Guiding Principles for the National
Guideline for supporting autistic
children and their families
- Occupational Therapy (e.g., noise cancelling headphones, a weighted toy dog or blanket to sit on the child’s lap)
- Sensory breaks
- Social stories
- Connecting with certain people or an animal on the school grounds
- Visual aids (e.g., visual schedules and visual learning strategies)
- Reducing sensory input (low lighting, a calm space to retreat to for respite)
- Appropriate use of technology
- Welcoming special interest toys (e.g., a Minecraft mat to sit on, bringing along a special interest toy to hold)
- Structured activities and support during unstructured play time
- Dohm White Noise Machine
- Drawing is an incredibly centring activity (e.g., have a sketchpad and pencil readily accessible)
- Rhythm and movement
- Relational co-regulation
If the child is overwhelmed (please see website link preventing meltdown escalating), help redirect the child to a quiet place by giving them a sense of purpose (e.g. feed the school chickens, take an important note the principal, help return a book to the library).
If the child is not eating at school, it may be helpful to allow them to eat during a different time when their is less sensory overwhelm. Autistic children will often experience a decreased appetite in highly stimulating environments. Autistic Children often exhibit restrictive food intake.

Please find below articles that may be of interest – ASD and Eating Disorders (ARFID-Avoidant Restrictive Food Intake Disorder).
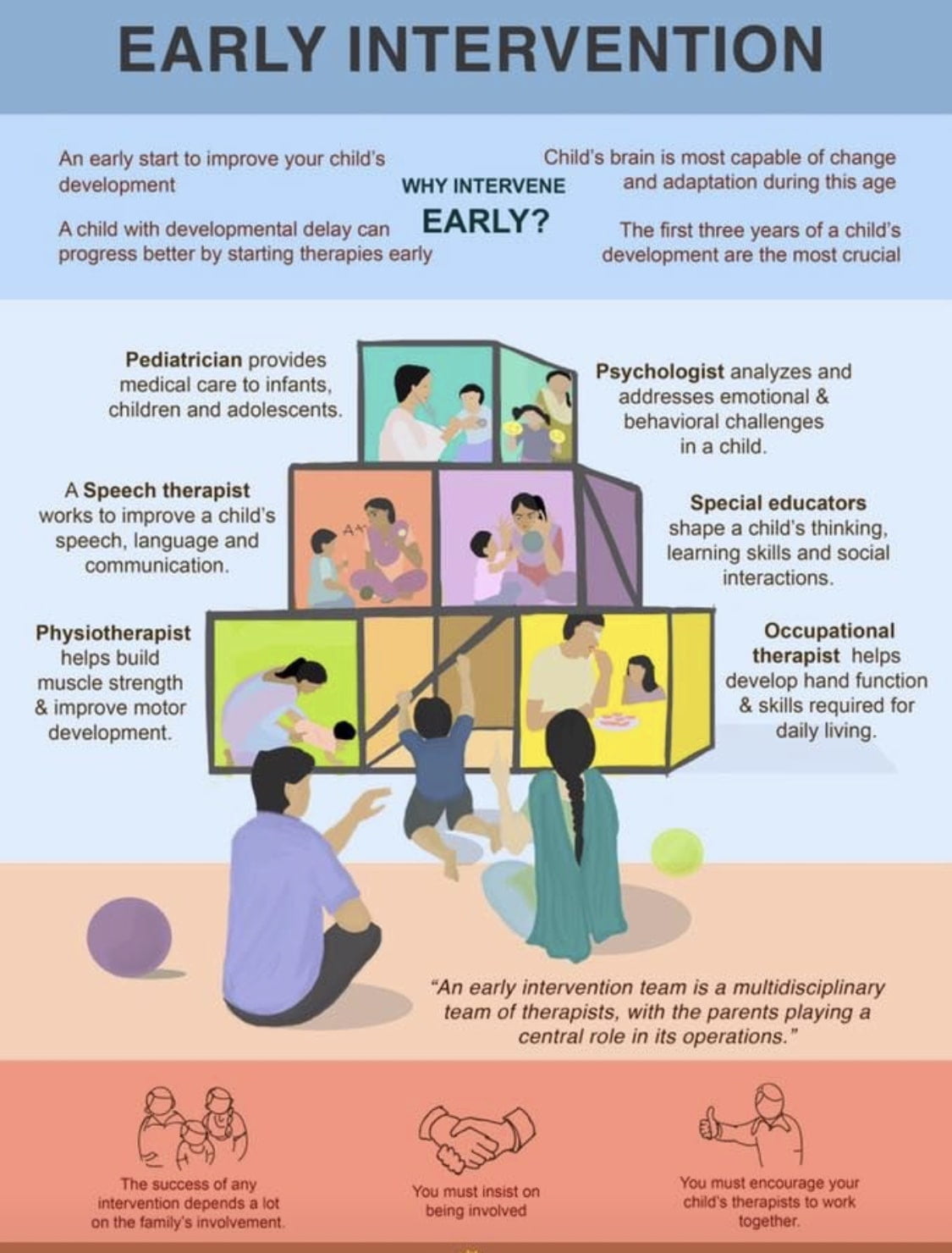
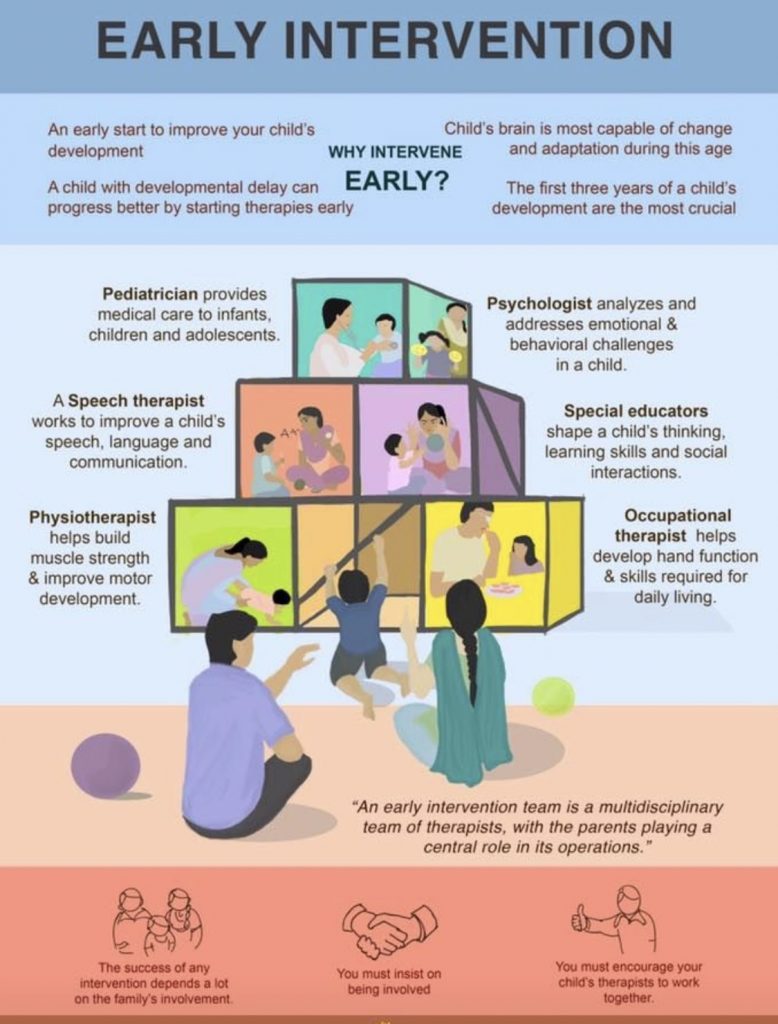
Early Intervention (Implemented by Allied Health Professionals and Educators)
Early intervention provides therapeutic treatment to promote; joint attention, sensory motor development, building skills in the area of completing daily and school activities, self-regulation skills, learning body clues for feelings, social thinking, perspective taking and more.
I would also like to add to the above early intervention team, the importance of group therapy that allows Autistic children to connect to their tribe.
Early Intervention (Implemented by Allied Health Professionals and Educators)
Early intervention provides therapeutic treatment to promote; joint attention, sensory motor development, building skills in the area of completing daily and school activities, self-regulation skills, learning body clues for feelings, social thinking, perspective taking and more.
This is by no means an exhaustive list however it gives an indication of therapeutic modalities that are demonstrating significant therapeutic outcomes with Autistic children.
- Mindfulness
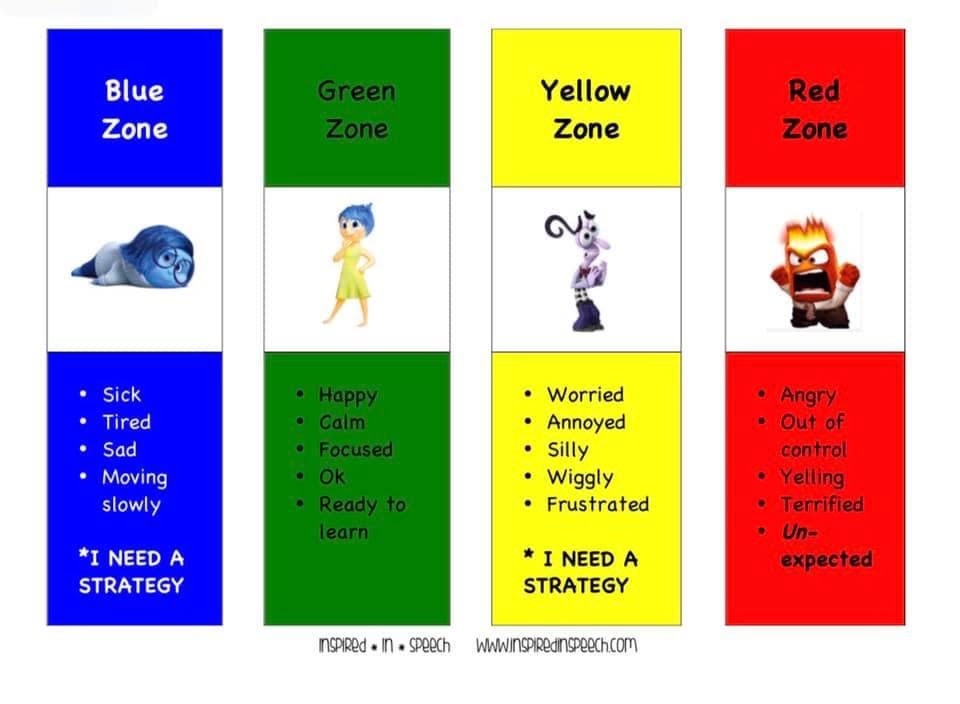
- The Zones of Regulation – by Leah M. Kuypers
- Meet Thotso, Your Thought Maker – by Rachel Robb Avery, Ph.D.; What is a Thought? – by Jack Pransky & Amy Kahofer
- Connecting with certain people or an animal on the school grounds
- Michelle Garica Winner coined the term “Social Thinking” in the mid-1990s and since that time has created numerous unique treatment frameworks and curricula that help educators and allied health professionals.
Professional Development
I highly recommend attending Events run by
http://autisticgirlsatschool.com.au/
Hill, E.L., & Berthoz, S. (2006). Response to “Letter to the editor: The overlap between alexithymia and Asperger’s Syndrome”. Fitzgerald and Bellgrove. Journal of Autism and Developmental Disorders, 36, 1143-1145.
Dziobek, I., Rogers, K., Fleck, S., Bahnemmann, M., Hauke, R., Heekeren, H.R., Wolf, O.T. & Convit, A. (2007). Dissociation of cognitive and emotional empathy in adults with Asperger Syndrome using multifaceted empathy test (MET). Journal of Autism and Developmental Disorders, 38, 464-473.
